
There has been a dramatic increase in the worldwide use of radio frequency (RF) technologies in the last two decades, especially in personal communications. In fact, since the introduction of commercial systems in 1983, cellular telephone service has been one of the fastest growing segments of the US telecommunications industry. By the end of 1984, cellular service had nearly 100,000 users. By the end of 1991, it had climbed to over two million users.1 Today, there are over 100 million hand-held cell phone users in the US. Because of this dramatic increase in the use of RF devices, there is an increasing concern over the biological effects of RF radiation from personal wireless communication devices; therefore, it is prudent to have on-going studies of health effects. The large number of cell phone users would lead to a major health problem if there were even a small hazard rate.
This article presents an overview of the biological effects of RF radiation, including safety issues and regulations. The interaction between handset antennas and biological tissues, quantified by the specific absorption rate (SAR), is explained. A discussion of the issue of health hazards associated with RF exposure is also presented, but the authors do not speculate whether or not low level RF radiation is harmful to humans. Even though it is widely believed that the use of mobile phones is safe, there are still many scientific studies and laboratory investigations being conducted that address potential health hazards of RF radiation from mobile phones.2,3
RF Radiation Basics
Electromagnetic waves are distinguished by their wavelength (λ) and frequency (f) (f = speed of light/λ). The RF portion of the electromagnetic spectrum is generally defined as that part of the spectrum where electromagnetic waves have frequencies in the range of 3 kHz to 300 GHz, as illustrated in Figure 1. The microwave portion (several hundred MHz to several GHz) of the spectrum is popular for commercial communication devices.
 | ||
| Fig. 1 The electromagnetic spectrum. | ||
Electromagnetic waves can be divided into two categories: ionizing and non-ionizing radiation. Ionization is the process by which electrons are stripped from atoms and molecules. This process can produce molecular changes that damage biological tissue, including effects on DNA. It requires high levels of electromagnetic energy. X- and Gamma-rays often have an energy level sufficiently high enough to ionize biological material. The energy levels associated with RF and microwave radiation, on the other hand, are rarely large enough to cause the ionization of atoms and are classified as non-ionizing radiation. Often the term radiation is applied to ionizing radiation such as that associated with nuclear power plants. Ionizing radiation should not be confused with lower energy, non-ionizing radiation with respect to possible biological effects, since their mechanisms are quite different.4 Non-ionizing radiation is discussed in this article.
Biological Effects and Health Issues
The mechanisms of non-ionizing electromagnetic radiation interaction with biological systems is grouped into two major types: thermal effects and non-thermal (or athermal) effects, depending on whether they are attributable to deposition of heat (thermal) or to a direct interaction of the EM field with the tissue substance without a significant heat component (non-thermal).
Thermal effects can occur in tissues as a result of EM field absorption in the dissipative tissue media. Radio frequencies cause water molecules and dissolved ions to vibrate, causing absorption. Water content is then an important parameter in determining the dielectric properties of biological tissues. An equivalent body tissue conductivity s is related to the imaginary part of the permittivity ε'' as:
σ = 2πfε'' [S/m] (1)
where
f = frequency of operation
Particularly in the microwave band, tissues having a high water content show a conductivity that increases with frequency. The absorbed power per unit volume (Pa) is proportional to the electric field in the material and its conductivity, such that

where
|![]() | = amplitude of the electric field
| = amplitude of the electric field
The RF energy actually absorbed in tissues is quantified using the specific absorption rate or SAR, the absorbed power per unit mass of tissue. SAR is the primary parameter used when discussing the health risk due to electromagnetic power absorption in the body and is defined as

where
ρ = material density in kg/m3
Non-thermal effects, on the other hand, are not caused by heat, but are due to direct interaction of the RF field with molecules and tissue components; the particles tend to orient themselves along the electric field such that potential energy is minimized.5 Non-thermal effects are not very well understood and their human health consequences are still under investigation.
A biological effect occurs when a biological change is measured in response to a stimulus. However, the observation of a biological effect does not necessarily suggest the existence of a biological hazard. A biological effect only becomes a safety hazard when it causes a detectable impairment of an individual’s health or offspring.4 There are many published reports in the scientific literature concerning possible biological effects resulting from RF energy exposure. These studies can be categorized into three types: cell studies, animal studies and epidemiological studies. Cell studies focus on single cells, multiple cells, or organs that are exposed to RF energy in a highly controlled exposure environment. Animal studies observe health changes or chemical effects in animals exposed to RF energy. Epidemiological studies examine a segment of the human population for relationships between health effects and RF exposure. Cellular studies can produce accurate results, but it is difficult to extrapolate conclusions from cellular response to effects on animals. Animal and epidemiological studies are subject to questions about controls during the study and the extraction of specific cause-effect relationships.
Thermal effects from RF radiation have been studied extensively in cells and animals, and it has been known for many years that exposure to very high levels of RF radiation can be harmful due to the ability of RF energy to rapidly heat biological tissue. In fact, microwave ovens cook food based on RF thermal effects. Exposure to very high RF field intensity produces heating in biological tissue and can increase body temperature. Fortunately, the intensity of radiation from hand-held devices is too low to cause such effects.
Non-thermal effects due to low RF radiation levels have also been investigated over the past two decades.6 However, evidence of harmful biological effects is ambiguous because results from these studies are often inconsistent or not replicated.6 Nonetheless, studies are ongoing, and key government agencies and industry organizations continue to monitor the results of the latest scientific research on this topic for using and setting safety guidelines for RF exposure.
RF Safety and Regulations
There are two parameters commonly used in RF radiation regulations: SAR and maximum permissible exposure (MPE). As discussed in the previous section, SAR relates to the absorption of RF radiation in biological tissues. MPE is the upper limit of RF radiation power density (mW/cm2) exposure for biological tissues.
RF exposure standards have been developed by various organizations and countries. These standards recommend safe levels of exposure for both the general public and workers. The recommended safe levels have been revised downward several times in recent years, but not all scientific bodies agree on safe levels. In the US, the Federal Communications Commissions (FCC) has adopted and used recognized safety guidelines for evaluating RF environmental exposure since 1985.4
Exposure standards are largely based on the thermal effects and are derived from absorption of plane waves by man or laboratory animals.4 The standards usually recommend RF exposure limits for two cases: controlled environment and uncontrolled environment. For the controlled environment case, energy levels are known and everyone in the exposure area is aware of the presence of electromagnetic fields (EMF). Also, personnel are expected to have received instruction in radiation safety and to have suitable approval protective clothing, or there is limited occupancy, in terms of time and distance, of the area. For uncontrolled environment (or general population), energy levels are not known or some people present may not be aware that they are exposed to EMF fields, including special risk groups, such as young children and pregnant women. The duration of exposure can also be substantially different in both groups.
The most popular recommendations are the ANSI/IEEE7 and the ICNIRP/CENELEC8 guidelines. The ANSI/IEEE C95.1-1992 guidelines7 for recommended EMF exposure limits went into effect in 1992 and were adopted by the FCC with some revisions. They replaced a 1982 ANSI guideline that permitted somewhat higher exposure levels. ANSI-recommended limits before 1982 were even higher.
For uncontrolled environments, the ANSI/IEEE C95.1-1992 standard suggests that: (a) the power density (mW/cm2) in the microwave frequency band, from 300 MHz to 15 GHz, should remain under f/1500, where f is the frequency of operation in MHz; (b) the SAR averaged over the whole body for 30 minutes or more should remain under 0.08 mW/g; and (c) the SAR averaged over any 1 gram of tissue for 30 minutes or more should remain under 1.6 mW/g. These recommended levels of exposure would raise the tissue temperature by no more than 1°C. However, the temperature increase rarely reaches 1°C, due to thermoregulation in the human body, and does not present an unacceptable thermal load, avoiding adverse effects on the functioning of the human body. The standard was not developed to protect against possible hazards from long-term exposure to low level RF radiation because such hazards are not well understood.
Figure 2 shows the maximum permissible exposure in terms of power density incident on a human for an uncontrolled environment in the frequency range from 100 MHz to 300 GHz recommended by the ANSI/IEEE standard and the ICNIRP/CENELEC European standard. Measurements, computational analysis using models of the human head and other studies of SAR distribution for hand-held cellular and PCS phones have shown that, in general, the 1.6 mW/g limit is unlikely to be exceeded under normal conditions of phone use.9
 | ||
| Fig. 2 Maximum permissible exposure (MPE) in terms of power density for uncontrolled environment 5 (© IEEE 2004 reprinted with permission). | ||
Human Operator Influence on Hand-held Radio Performance
There are two reasons for understanding the effects of electromagnetic fields radiated from mobile phones in the presence of the user’s head and hand. The first reason is related to the antenna/handset design because the presence of a user influences the radiation characteristics of a mobile phone. The presence of the hand and head can be taken into account at an early stage of mobile phone design. The second reason to understand interaction effects is for compliance with safety standards by examining dosimetry aspects to evaluate the SAR inside the head and inside the hand, which are then compared to permitted levels. Interaction studies can be performed both by computation and by measurements. There are various computational methods to perform numerical studies. The finite-difference time-domain (FDTD) computational method is often used for such a numerical evaluation process, and its implementation is briefly discussed in the next section.
Computational Simulation
The FDTD numerical method of computational simulation is very well suited for evaluating large and inhomogeneously-filled computational domains, and is widely used for analyzing the coupling of mobile communication equipment and the human head that are in close proximity. FDTD is based directly on the differential form of time-domain Maxwell’s equations, and material parameters ε, μ and σ, which are the space-dependent permittivity, permeability and conductivity, respectively. The entire problem space is gridded in both spatial and temporal dimensions. The details of this process were originally formulated in the 1960s by Yee10, and are summarized by Stutzman, et al. [11, chap. 9] Once the time-domain computation using this method is completed, a Fourier transform is performed to obtain the desired frequency-domain quantities such as input impedance, radiation pattern and gain.
Electromagnetic Modeling of the Human Operator
The SAR is measured directly as a temperature increase in a localized area of tissue, as quantified later in Equation 4. Measuring SAR directly is nearly impossible in practice because it is necessary to insert calorimetric probes into a live human head tissue. As a result, head models with mathematical simulations (or measurement using physical head models) are used for estimating SAR.
Over the past ten years, there have been many studies that model biological tissues such as the human hand and head.12–26 Simple models of human tissues were realized first. For instance, the human hand was modeled as a layer of bone surrounded by a layer of muscle. The human head (see Figure 3) was first represented by a rectangular box or a sphere with homogeneous material. With the advances in computational methods and in computation speed, the human body models became more complex and accurate by including more types of tissue layers. With the help of magnetic resonance imaging (MRI), very realistic human hand and head models were finally obtained. Table 1 presents values of relative permittivity, conductivity and density of tissues in the hand and head near 900 MHz.12
 | ||
| Fig. 3 Popular human head models used in numerical simulations; (a) simple models, (b) the Multi-layered Model12 and (c) complex model based on MRI data. | ||
 | ||
As the degree of the biological tissue model complexity increases, the computer performance requirement also increases. Thus, it is important to employ only the level of modeling complexity that is necessary for accurate results. Okoniewski and Stuchly16 compared various simple models with complex ones from the Yale School of Medicine and the University of Gent in Belgium. Table 2 summarizes their computed values of antenna efficiency, η, which is the ratio of the power radiated to the power input to the antenna, and power absorbed, Pabs, in the head for a handset with a monopole antenna located 1.5 cm from the head. Two issues were investigated in the paper: the utility of the simplified canonical models and the significance of a more realistic model of the head. The important conclusion that can be drawn from Table 2 is that spherical models provide estimates of the antenna efficiency and total absorbed power in the head that are in reasonably good agreement with non-homogeneous complex model predictions. However, the very simple box model is inadequate.
 | ||
In the past decade, laboratory human head body models, called phantoms, have been developed for experimental investigations. Again, there are various degrees of complexity in the phantoms, ranging from a simple geometric shape to realistic human body shapes where the interior is filled with one or more liquids with dielectric properties equivalent to those of human body at the frequencies under consideration. With the help of phantom models, experimental determination of SAR is possible.
Human Operator Effects on Antenna Characteristics
The data shown in Table 2 indicates that the efficiency of a monopole antenna located 1.5 cm from the head at 900 MHz is roughly 50 percent. This means that the human head absorbs about half of the power radiated from the monopole antenna. Table 3 illustrates additional results for the power absorbed in the head as function of the separation distance between the head and the antenna, giving the expected result that efficiency increases with distance from the head and, thus, power absorbed in the head decreases.
 | ||
The effects of power absorption on the far-field radiation pattern of the antenna are shown in Figure 4. The patterns were obtained from simulations of a monopole on a rectangular box model for the handset located 1.5 cm from the head for three levels of model complexity using Fidelity from Zeland (www.zeland.com). The results demonstrate that the omni-directional pattern is radically altered by the presence of the human head. The pattern for the sphere model case is very similar to the one for the Yale anatomical head model,15 which is considered to be the most accurate. It is not surprising that the box model results are less accurate than the sphere model because the box representing the head nearly entirely blocks the radiation in the head direction. In the case of a sphere, there is less dramatic but significant reduction in power radiated towards the half-space in the direction of the head (φ = 0°). The pattern for the spherical head model shows that radiation is reduced by more than 10 dB over a wide angular region in the horizontal plane.
 | ||
| Fig. 4 Computed radiation patterns in φ plane (θ = 90°) for a monopole oriented along the Z-axis at F = 900 MHz. | ||
The influence of the human operator on input impedance must also be considered in antenna design because the overall efficiency is reduced with increasing impedance mismatch. In fact, with a large impedance mismatch, only a small amount of power from the source is delivered to the antenna when transmitting, and only a small portion of the power is transferred from the antenna when receiving. The effects of biological tissues on the input impedance for two antenna types and configurations have been studied. In contrast to human operator influence on the radiation pattern of a monopole, there is relatively little influence on the antenna input impedance, as illustrated in Figure 5, which shows the computed return loss of a monopole with and without biological tissues in proximity. This is a desirable characteristic of the monopole, which partly accounts for its widespread use. For conformal and internal antennas, such as the planar inverted-F antenna (PIFA), dramatic detuning can occur due to hand and/or head presence. An example of such an effect can be seen for the PIFA antenna described in Figure 6. Figure 7 shows the return loss for the PIFA antenna for several operator configurations. A return loss of 10 dB (approximately equivalent to VSWR = 2) or more is the commonly accepted limit for impedance mismatch. The plot compares the results with no biological tissue included to those when a hand is placed at three vertical locations on the handset. The hand detunes the antenna operating frequency and introduces impedance mismatch. A high impedance mismatch occurs when the hand begins to mask the antenna. These results show the importance of minimizing the antenna masking through proper antenna placement on the handset.
 | ||
| Fig. 5 Computed return loss values of a monopole on a handset for three cases. | ||
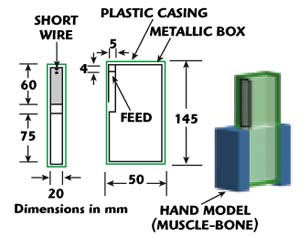 | ||
| Fig. 6 Handset model showing the PIFA antenna location and the hand model used in the return loss computations. | ||
 | ||
| Fig. 7 Computed return loss of the side-mounted PIFA handset for different hand locations. | ||
Power Absorption in the Head and SAR
As previously mentioned, radiation exposure standards are based on the thermal effects of RF radiation, specifically the RF power absorbed in the head. SAR is expressed in units of watts per kilogram (W/kg) and is the fundamental parameter used to examine health risks of electromagnetic power absorption in the head. SAR is a point quantity that varies with location and, thus, is used to both locate and quantify regions of high absorption in the human operator. The accuracy and reliability of a given SAR value depends on the accuracy of three key parameters: tissue density, tissue conductivity and the electric field level present, the most significant of which is the induced electric field.
RF-power absorption in biological tissue causes the tissue’s kinetic energy to increase with exposure duration. If the incident power density is sufficiently high, the absorbed RF energy will produce a temperature increase. The rate of increase of temperature is proportional to the SAR value found using
![]()
where
c = specific heat of the tissue (J/kg per °C)
ΔT = transient temperature rise (°C)
Δt = duration (s) of power application used in the linear portion of the temperature rise. At the start of exposure, temperature rise is linear with time.27
If the entire body is exposed to the radiation, the average SAR is defined as the ratio between the total power absorbed and the mass of the whole body. When a part of the body is exposed to radiation, the SAR is also evaluated for a reference mass (for example, 10 g). A higher SAR level can be tolerated locally, provided that the allowed average SAR is not exceeded. Popular standards of electromagnetic radiation exposure limits for the general public are summarized in Table 4. Allowed SAR values vary with the mass of tissue used in the standard (1 g for IEEE standards, and 10 g for CENELEC and ICNIRP). The distribution of absorbed microwave energy varies greatly from point to point inside the user’s head. Therefore, a larger averaging mass (such as 10 g) smooths the computed or measured SAR distribution, tending to lower the averaged value by a factor of two or three for the same exposure over a smaller mass (such as 1 g).28 For example, a 10 g SAR of 2 W/kg (mW/g) is equivalent to a 1 g SAR of 4 to 6 W/kg (mW/g). In other words, the absorbed power averaged over a tissue mass of 10 g is low compared to a 1 g SAR value. The 1 g SAR quantity is a more precise spatial measure of localized microwave-power absorption, providing a detailed distribution of power absorbed inside the head. The SAR values for a mobile phone human operator exposure to microwaves vary with simulation model sophistication and depend on individual operator habits.
 | ||
Most cellular telephones sold in North America are in compliance with FCC rules and regulations; however, at present, there does not exist a standard testing protocol for measuring SARs for mobile phones. Some variations in measured SAR values were as large as 100 percent for the same telephone.27 In addition to the phantom head model used, the measurement technique and the instrumentation, SAR values also depend on the orientation of the handset, its tilt angle from vertical, the geometry of the ear and the handset antenna to head separation distance.
Conclusion
With the progress in computational electromagnetics and the advancement in biological research, one can expect more accurate and conclusive results for biological effects on human tissues due to low level microwave radiation from portable wireless devices. Unlike pollution of the environment where there is a tradeoff between public health and commercial development, the goal for wireless communications is to improve performance by reducing the power absorbed in the user’s body. This increases the signal to distant points for the same transmitter power. Thus, both communication performance and health hazard conditions are improved.
The study of microwave exposure requires collaboration between engineers and medical professionals. Understanding how operator presence affects antenna performance and the associated health hazards aids engineers to develop hand-held wireless products that minimize operator exposure and improve antenna radiation efficiency. Also, biologists can have a better understanding of low level electromagnetic radiation in human tissues with the help of more accurate electromagnetic propagation models in complex inhomogeneous media.
There is no widely accepted relationship between microwave exposure and health effects. The preponderance of evidence suggests that there is no health hazard due to long-term low level exposure to handset radiation.21 However, due to the pervasiveness of cell phone use, it is prudent to continue investigating potential health problems.
References
- US Government Accounting Office, “Telecommunications: Concerns About Competition in the Cellular Telephony Industry,” GAO/CED-92-220, July 1992.
- J.C. Lin, “Cell Phone Testing and Fundamental Scientific Research,” IEEE Antennas and Propagation Magazine, Vol. 43, No. 4, August 2001, pp. 156–158.
- J.C. Lin, “Cellular Telephone Radiation and Electroencephalograms (EEG),” IEEE Antennas and Propagation Magazine, Vol. 45, No. 5, October 2003, pp. 150–153.
- R.F. Cleveland, Jr. and J. Ulcek, “Questions and Answers about Biological Effects and Potential Hazards of Radiofrequency Electromagnetic Fields,” OET Bulletin 56, Fourth Edition, FCC/OET, August 1999.
- A. de Salles, “Biological Effects of Microwave and RF,” SBMO/IEEE MMT-S IMOC’99 Proceedings, April 1999, pp. 51–56.
- R. Goldberg, “Literature Resources for Understanding Biological Effects of Electromagnetic Fields,” EMF-link Multimedia Resource, http://infoventures.com/ emf/top/lit-rev.html.
- American National Standards Institute (ANSI), “IEEE C95.1-1992: IEEE Standard for Safety Levels with Respect to Human Exposure to Radio Frequency Electromagnetic Fields, 3 kHz to 300 GHz,” The Institute of Electrical and Electronics Engineers Inc., 1992.
- ICNIRP Guidelines, “Guidelines for Limiting Exposure to Time-varying Electric, Magnetic and Electromagnetic Fields (up to 300 GHz),” International Commission on Non-ionizing Radiation Protection, Health Physics, Vol. 74, No. 4, April 1998, pp. 494–522.
- FCC/OET, “Information on Human Exposure to Radiofrequency Fields from Cellular and PCS Radio Transmitters,” January 1998.
- K.S. Yee, “Numerical Solution of Initial Boundary Value Problems Involving Maxwell’s Equations in Isotropic Media,” IEEE Transactions on Antennas and Propagation, Vol. 14, May 1966, pp. 302–307.
- W.L. Stutzman and G.A. Thiele, Antenna Theory and Design, Second Edition, John Wiley & Sons Inc., 1998.
- M.A. Jensen and Y. Rahmat-Samii, “EM Interaction of Handset Antennas and a Human in Personal Communications,” Proceedings of the IEEE, Vol. 83, No. 1, January 1995, pp. 7–17.
- O.P. Gandhi, J.Y. Chen and D. Wu, “Electromagnetic Absorption in the Human Head for Mobile Telephones at 835 and 1900 MHz,” Proceedings of the International Symposium Electromagnetism and Compatibility, Rome, Italy, Vol. 1, September 1994, pp. 1–5.
- J. Toftgard, S.N. Hornsleth and J.B. Andersen, “Effects on Portable Antennas in the Presence of a Person,” IEEE Transactions on Antennas and Propagation, Vol. 41, No. 6, June 1993, pp. 739–746.
- S. Watanabe, M. Taki, T. Nojima and O. Fujiwara, “Characteristics of the SAR Distribution in the Head Exposed to Electromagnetic Field Radiated by a Hand-held Portable Radio,” IEEE Transactions on Microwave Theory and Techniques, Vol. 44, No. 10, October 1996, pp. 1874–1883.
- M. Okoniewski and M.A. Stuchly, “A Study of the Handset Antenna and Human Body Interaction,” IEEE Transactions on Microwave Theory and Techniques, Vol. 44, No. 10, October 1996, pp. 1855–1874.
- L.W. Li, et al., “FDTD Analysis of Electromagnetic Interactions Between Handset Antennas and the Human Head,” Asia-Pacific Microwave Conference Proceedings, 1997, Vol. 3, December 2–5, 1997, pp. 1189–1192.
- C.W. Trueman, “Validation of FDTD Handset and Head Patterns by Measurement,” Antennas and Propagation for Wireless Communications, IEEE-APS Conference, November 1998, pp. 93–96.
- K. Ito, Y. Okano, A. Hase and I. Ida, “A Tissue-equivalent Solid Phantom for Estimation of Interaction Between Human Head and Handset Antenna,” Proceedings of IEEE APS Conference on Antennas and Propagation for Wireless Communications, November 1998, pp. 89–92.
- N. Kuster, “Radiation Performance and Evaluation of Human Exposure from Mobile Handsets Using Near-field Measurements,” Proceedings of the International Symposium on Electromagnetic Compatibility, May 1999, pp. 480–483.
- K.R. Foster and J.E. Moulder, “Are Mobile Phones Safe?,” IEEE Spectrum, Vol. 37, No. 8, August 2000, pp. 23–28.
- K. Nikita, et al., “A Study of Uncertainties in Modeling the Handset Antenna and Human Head Interaction Using the FDTD Method,” IEEE International Microwave Symposium Digest, Vol. 2, December 2000, pp. 1025–1028.
- A. Drossos, V. Santomaa and N. Kuster, “The Dependence of Electromagnetic Energy Absorption Upon Human Head Tissue Composition in the Frequency Range of 300-3000 MHz,” IEEE Transactions on Microwave Theory and Techniques, Vol. 48, No. 11, November 2000, pp. 1988–1995.
- J. Moustafa, “Investigations of Reduced SAR Personal Communications Handset Using FDTD,” Proceedings of IEE Eleventh International Conference on Antennas and Propagation, 2001, Vol. 1, April 2001, pp. 11–15.
- M. Francavilla, A. Schiavoni and G. Richiardi, “Effect of the Hand on Cellular Phone Radiation,” IEEE Proceedings on Microwave Antennas and Propagation, Vol. 148, No. 4, August 2001, pp. 247–253.
- N. Chavannes, et al., “Suitability of FDTD-based TCAD Tools for RF Design of Mobile Phones,” IEEE Antennas and Propagation Magazine, Vol. 45, No. 6, December 2003, pp. 52–66.
- J.C. Lin, “Specific Absorption Rates (SARs) Induced in Head Tissues by Microwave Radiation from Cell Phones,” IEEE Antennas and Propagation Magazine, Vol. 42, No. 5, October 2000, pp. 138–139.
- P. Bernardi, M. Cavagnaro, S. Pisa and E. Piuzzi, “Specific Absorption Rate and Temperature Increases in the Head of a Cellular Phone User,” IEEE Transactions on Microwave Theory and Techniques, Vol. 48, No. 7, July 2000, pp. 1118–1126.
Minh-Chau T. Huynh received his BS and MS degrees in electrical engineering from Virginia Polytechnic Institute and State University in 1997 and 2000, respectively. He is currently pursuing his PhD degree in electrical engineering from the same university. Since 1997, he has been with the department of electrical and computer engineering at Virginia Tech as a research assistant. He joined the Virginia Tech Antenna Group in December 1998. His research interests include wideband low profile compact antennas and ultra-wideband antennas.
Warren L. Stutzman received his BS degree in electrical engineering and his AB degree in mathematics from the University of Illinois in 1964 and his MS and PhD degrees in electrical engineering from Ohio State University in 1965 and 1969, respectively. He has been on the electrical engineering faculty of Virginia Polytechnic Institute and State University since 1969 and is currently the Thomas Phillips Professor of Engineering. He served as the director of the Antenna Group from its beginning in 1983 until 2001. His research activities include antennas for wireless systems, propagation, reflector antennas, phased array design and atmospheric effects on earth-space communication links. He has authored over 75 journal articles. He is co-author of the textbook Antenna Theory and Design (John Wiley & Sons Inc., 1981) and wrote Polarization in Electromagnetic Systems (Artech House Inc., 1993). He is a fellow of the IEEE and served as president of the IEEE Antennas and Propagation Society in 1992.